




At 1:12 a.m., someone refreshes their group chat. A friend is live-texting a glossy TV finale—high stakes, big feelings, a “bold new era” vibe that’s been all over entertainment coverage lately. Another message lands: “Also… we’re thinking about trying this month. At home.”

That quiet pivot is happening everywhere. Between celebrity pregnancy chatter, headlines about pregnancy loss storylines being handled differently on-screen, and the general cultural obsession with “who’s expecting,” real people are still doing the unglamorous work: choosing a path, managing risk, and figuring out what’s realistic.
This guide is about ICI (intracervical insemination) using a home insemination kit. It’s direct, safety-first, and focused on what to document so you don’t create avoidable medical, legal, or emotional mess.
Is at-home insemination (ICI) actually a real option?
Yes—ICI is a real method people use at home, especially when they want privacy, lower costs than clinic procedures, or a gentler entry point before exploring IVF.
That said, “real option” doesn’t mean “right for everyone.” ICI relies heavily on timing and sperm quality, and it doesn’t bypass issues like blocked tubes. If you’re unsure about underlying factors, a clinician can help you avoid months of guessing.
What ICI is (and isn’t)
- ICI: Semen is placed near the cervix. It’s typically less invasive and can be done at home.
- Not IUI: IUI places prepared sperm into the uterus and is performed in a medical setting.
- Not IVF: IVF involves eggs, lab fertilization, and embryo transfer. Different level of testing, monitoring, and cost.
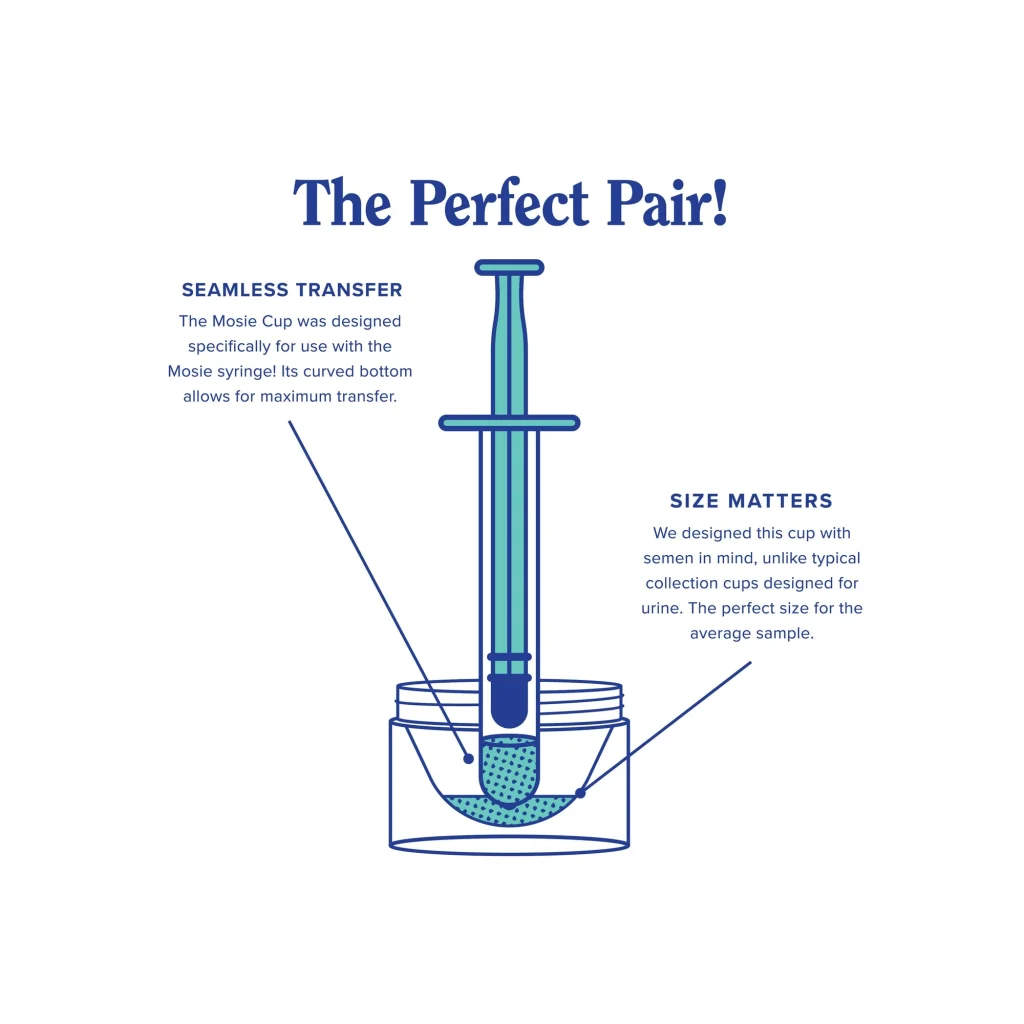
What should a home insemination kit include (and what should you avoid)?
People get tripped up by “DIY” shortcuts. Clean technique and the right materials matter because infection risk is not a vibe—it’s a real complication.
Look for basics that support safer handling
- Single-use, sterile syringes designed for this purpose (not needles).
- Clear, simple instructions you can follow without improvising.
- Packaging that protects sterility until use.
Avoid common mistakes that raise risk
- Reusing anything that should be single-use.
- Using household containers that aren’t sterile.
- Using lubricants not labeled fertility-friendly (some can harm sperm).
- Ignoring pain, fever, unusual discharge, or foul odor—those are reasons to stop and seek care.
If you’re comparing options, you can start with this at-home insemination kit for ICI search-style overview and match it against the checklist above.
How do people time ICI at home without turning it into a second job?
Timing is the make-or-break variable for many couples and solo parents by choice. You don’t need a wall of spreadsheets, but you do need a plan you can repeat.
Keep it simple: pick one tracking approach and stick with it
- Ovulation predictor kits (OPKs): Often used to identify the LH surge.
- Cervical mucus observations: Some people pair this with OPKs for more context.
- Basal body temperature (BBT): Helpful for confirming ovulation after the fact.
If cycles are irregular, timing can get murky fast. That’s a good moment to talk with a clinician instead of forcing a “just try harder” approach.
What safety screening matters most before trying at home?
On TV, pregnancy plots can change with a rewrite. In real life, prevention is the rewrite you want. The goal is to reduce avoidable infection and to make sure everyone understands the medical and legal stakes.
Health screening and hygiene basics
- Consider STI testing for all involved, especially with a new or known donor arrangement.
- Use sterile supplies and wash hands thoroughly before handling anything.
- Don’t proceed if someone has symptoms of infection or unexplained pelvic pain.
Donor and consent documentation (don’t skip this)
- Write down what was agreed: donor role, contact expectations, and boundaries.
- Keep a dated record of each attempt (timing method, any symptoms, and supplies used).
- Consider legal advice for known-donor situations. Laws vary widely by location.
Even if you’re a “paperwork makes me anxious” person, documentation protects relationships. It also helps a clinic later if you decide to escalate care.
When does it make sense to move from ICI to a clinic or IVF?
It’s normal to start at home and later want more support. The switch isn’t a failure; it’s a decision based on time, data, and emotional bandwidth.
Common reasons people level up care
- Repeated cycles without success and no clear explanation.
- Known conditions that make ICI less likely to work (for example, tubal factors).
- Need for donor sperm processing, monitoring, or specific testing.
- Desire for a structured plan with medical oversight.
Some people also lean on tech to organize attempts, predict fertile windows, or track patterns. If you’re curious about what “AI” means in that context, here’s a neutral reference: home insemination kit.
Common questions people ask right now (and why)
Between celebrity bump-watch lists and entertainment coverage debating how pregnancy loss is portrayed, it’s easy to feel like everyone else has a clear path. Most don’t. These are the questions that come up in real conversations.
“Is trying at home less stressful?”
It can be, because you control the setting and schedule. It can also feel isolating if you don’t have support or a plan. A simple checklist reduces decision fatigue.
“How do we keep it private but still responsible?”
Privacy and responsibility can coexist. Use sterile supplies, screen for infections, document consent, and know your local legal landscape—especially with known donors.
“What if the story gets complicated?”
Fertility journeys can include disappointment and loss. If you’re coping with grief, anxiety, or relationship strain, consider mental health support alongside medical guidance. You deserve care that isn’t only about logistics.
Medical disclaimer: This article is for general education and is not medical or legal advice. It does not diagnose or treat any condition. For personalized guidance—especially about infections, fertility conditions, donor agreements, or pregnancy loss—consult a qualified clinician and/or attorney.