Fertility talk is everywhere right now. Some of it feels like a rom-com montage, and some of it reads like courtroom drama.

If you’re trying to get pregnant, you don’t need more noise. You need a plan that doesn’t waste a cycle.
This guide helps you decide when a home insemination kit makes sense for ICI, when to consider a clinic, and what to think about before you start.
A quick reality check (before the decision tree)
At-home insemination (ICI) is a practical option for many couples and solo parents, especially when intercourse isn’t working for logistical, medical, or personal reasons. It can also be a first step before moving to IUI or IVF.
Still, it isn’t a magic shortcut. Timing, sperm quality, and underlying fertility factors matter. Budget matters too, because repeating attempts gets expensive fast.
Decision guide: If…then… choose your next step
If your cycles are fairly predictable, then start with ICI at home
If you usually ovulate in a recognizable window and you can track it, ICI may be a reasonable first-line option. It’s often lower cost than clinic procedures and easier to repeat across a few cycles.
Focus on two things: (1) accurate timing, and (2) a setup that reduces mess and stress. You want the process to feel routine, not like a high-stakes event.
If timing feels like a moving target, then tighten tracking before you spend more
If your cycles vary a lot, your first “upgrade” may be better tracking rather than jumping straight to IVF. Many people use ovulation predictor kits plus a simple tracking method to spot patterns.
When you’re unsure of ovulation, it’s easy to burn through attempts. That’s the budget trap. Better data can save you more than a new procedure.
If you’re using a known donor, then treat the legal side like a real step
Pop culture loves a twist ending. Real life doesn’t need one.
Recent coverage about court decisions has put a spotlight on how at-home insemination arrangements can raise parentage questions, especially when documentation is informal. If you’re using a known donor, consider getting legal guidance in your area before you begin.
For a general reference point on what’s being reported, see this update: Florida Supreme Court makes ruling in at-home artificial insemination case.
If you’re 35+ (or approaching it), then avoid the panic and pick a timeline
One number gets repeated so often it starts to feel like a deadline: 35. The more accurate framing is this: fertility changes over time, but it’s not a light switch that flips overnight.
If age is part of your decision, the most helpful move is setting a time-box. Example: “We’ll try ICI for X cycles with solid tracking, then reassess with a clinician.” That keeps you from drifting month to month.
If you’ve tried several well-timed cycles, then consider an evaluation and clinic options
If you’ve done multiple attempts with good timing and no pregnancy, you may be better served by medical input than by repeating the same plan. A clinician can discuss labs, ultrasound monitoring, semen analysis, and whether IUI or IVF is a better next step.
Think of it like choosing what to watch next. A light movie list can be fun, but if you’re stuck in the same plot, it’s time to change the genre.
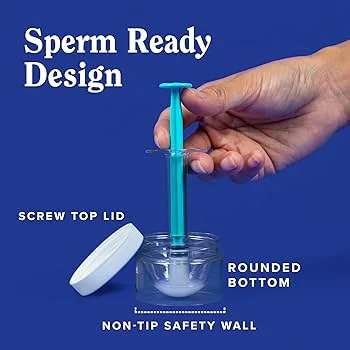
What a home insemination kit is (and what it isn’t)
A home insemination kit is designed to help place semen near the cervix (ICI) with less mess and more control than improvising. It’s not the same as a clinic procedure, and it doesn’t replace medical care for known fertility conditions.
Look for body-safe materials, clear instructions, and single-use or properly sanitizable components. Comfort matters, because tension can make the process harder than it needs to be.
Mini checklist: reduce wasted attempts this cycle
- Confirm your window: Use OPKs and track symptoms for at least one cycle if you’re unsure.
- Plan logistics: Decide the day/time, privacy, and cleanup plan ahead of time.
- Keep it gentle: Avoid anything that could irritate tissue or introduce bacteria.
- Document basics: Dates, OPK results, and any relevant notes help you improve next cycle.
- Set a reassessment point: Choose how many tries you’ll do before changing strategy.
FAQs (quick answers)
Is ICI the same as IUI?
No. ICI is done at home near the cervix. IUI is done in a clinic and places washed sperm in the uterus.
Do home insemination kits work?
They can, depending on timing and individual factors. If you’re not seeing results after several well-timed attempts, consider medical evaluation.
What’s the best timing for ICI?
Many aim for the day before and the day of ovulation. OPKs can help identify the surge that typically occurs shortly before ovulation.
Is at-home insemination legal?
It depends on your location and your documentation. Informal known-donor arrangements can create legal risks, so consider professional guidance.
Is 35 a hard fertility cliff?
No. Fertility is influenced by multiple factors and changes over time. If age is a concern, set a clear timeline and reassess with a clinician.
Medical disclaimer
This article is for educational purposes only and isn’t medical or legal advice. It does not diagnose or treat any condition. If you have known fertility concerns, severe pain, fever, unusual bleeding, or questions about infection risk or parentage, talk with a qualified clinician and/or attorney.
CTA: Keep it simple, keep it repeatable
If you’re leaning toward ICI, choose tools that help you stay calm and consistent. The goal is a clean, comfortable attempt you can repeat without dread.
How does at-home insemination (ICI) work?
Ready to compare options? Start here: at-home insemination kit for ICI.