Before you try at-home ICI, run this checklist.

- Timing: you have a plan for your fertile window (not just a guess).
- Supplies: you’re using a home insemination kit designed for the job.
- Screening: you’ve thought through infection risk and testing.
- Paperwork: you’ve addressed consent and parentage questions early.
- Backup: you know when you’ll escalate to a clinic.
At-home insemination (ICI) is having a cultural moment. Pregnancy storylines keep showing up in TV and film, and celebrity baby buzz can make it feel like conception is always quick and tidy. Real life is messier. It’s also more practical than people think, as long as you treat safety and legal clarity as part of the plan.
Medical disclaimer: This article is educational and not medical or legal advice. It can’t diagnose conditions or replace care from a licensed clinician or attorney.
A fast decision guide: if…then…
If you want the lowest-intervention option, then start with ICI basics
ICI (intracervical insemination) is often chosen because it’s less complex than clinic procedures. The goal is simple: place semen near the cervix around your fertile window and let biology do the rest.
If you’re comparing ICI to IVF as “home vs clinic,” remember the trade-off. IVF can add testing and lab support. ICI can add privacy and lower cost, but it puts more responsibility on you for timing, cleanliness, and documentation.
If timing feels like the main stressor, then simplify it
Many people spiral on timing. They track five apps, read ten forums, and still feel unsure. A calmer approach is to pick one primary method, then stick with it for a cycle or two.
Some people use an ovulation calculator as a starting point, then confirm with body signs or ovulation tests. If your cycles are irregular, a calculator may be less reliable, and clinician input can save time.
If you’re using a known donor, then treat “legal” like a safety step
Recent reporting has put a spotlight on Florida, where court decisions and related commentary have raised public awareness that at-home arrangements can create real legal exposure. The headline takeaway is not “panic.” It’s “don’t assume.”
In plain terms: when insemination happens outside a clinic, parentage rules may be less clear. If you’re using a known donor, talk to a family law attorney in your state before you start. Do it even if everyone is friendly today.
To see the broader coverage people are discussing, read: Florida Supreme Court makes ruling in at-home artificial insemination case.
If you’re worried about infection risk, then tighten your process
Safety is not about being “perfect.” It’s about reducing avoidable risk. Use sterile, single-use supplies and avoid improvised tools not intended for insemination.
Screening is also part of safety. If you’re using donor sperm, consider how testing is handled and documented. If anything feels vague, slow down and get clarity first.
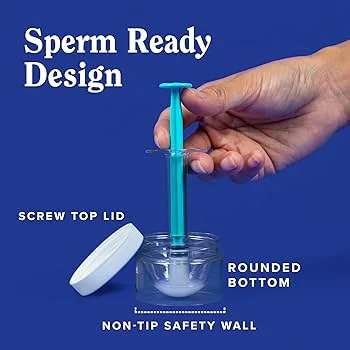
If you’re choosing supplies, then avoid the “random cart” approach
The internet makes it easy to buy a mix of items that don’t fit together. A purpose-built kit can remove guesswork and reduce contamination risk from mismatched or non-sterile components.
If you’re shopping, start here: at-home insemination kit for ICI.
If you’re on attempt #3+ and feeling stuck, then set a clear escalation point
TV dramas can make conception look like a single-episode plot twist. In reality, it can take time even when everything is “right.” Still, you deserve a plan that protects your mental bandwidth.
Pick a number of well-timed cycles after which you’ll seek a fertility consult. This is especially important if you’re older, have irregular cycles, or have known reproductive health concerns.
What to document (so future-you isn’t blindsided)
- Consent: who agrees to what, and when.
- Intended parentage: who will be the legal parent(s).
- Donor expectations: contact, boundaries, and future disclosure.
- Testing/screening notes: what was done, and where records live.
If you’re thinking, “This feels like paperwork for something personal,” you’re not wrong. It’s also one of the best ways to keep a hopeful process from turning into a legal or relational mess later.
FAQ (quick answers)
Is ICI the same as IVF?
No. ICI supports natural fertilization; IVF uses lab fertilization and embryo transfer.
Can an at-home sperm donor have parental rights?
Possibly, depending on your jurisdiction and the facts. Florida headlines have highlighted that home insemination can create legal disputes. Get state-specific advice.
How do I reduce infection risk at home?
Use sterile, single-use supplies and avoid non-medical tools. Pause and seek care if you have symptoms of infection.
Do I need an ovulation calculator?
It can help estimate your fertile window. If cycles are irregular, consider additional methods or clinician guidance.
Next step
If you want a more controlled, less improvised setup, choose a kit designed for ICI and pair it with a timing plan and documentation.