


On a Tuesday night, an anonymous couple sits on the edge of the bed with a phone timer, a sticky note that says “LH surge,” and a dozen tabs open. One tab is celebrity pregnancy chatter. Another is a debate thread about whether “35” is a hard deadline. A third is a news story about a court decision involving at-home insemination.

They aren’t trying to recreate a clinic. They just want a clean, repeatable plan that doesn’t turn every cycle into a spiral. If that’s you, this guide breaks down ICI (intracervical insemination) at home with a focus on timing, supplies, and simple steps.
Quick overview: what ICI at home is (and isn’t)
ICI is a way to place sperm near the cervix around ovulation. People use it when intercourse isn’t possible, when using donor sperm, or when they want a more controlled attempt at home.
It’s not IVF. IVF is a medical process with egg retrieval, lab fertilization, and embryo transfer. You may see headlines about research pushing IVF forward in unexpected places (even in veterinary settings). The cultural takeaway is simple: fertility science is advancing, but most people still need practical, accessible options right now.
Medical note: This is general education, not medical advice. It can’t diagnose fertility issues or replace care from a licensed clinician.
Timing that actually matters: your fertile window, simplified
If you only optimize one thing for ICI, make it timing. Most “failed” cycles are really “missed window” cycles.
Use two signals, not ten
- LH ovulation tests: A positive often means ovulation may happen in the next ~12–36 hours (varies by person).
- Cervical mucus changes: Many people notice more slippery, clear, stretchy mucus as ovulation approaches.
When those line up, you’re close. That’s the moment to stop doom-scrolling and start the plan.
A simple timing plan for ICI
- Best targets: The day before ovulation and the day of ovulation.
- If you only do one attempt: Aim for the day you get a strong LH positive or within the next day, depending on your typical pattern.
About the “fertility cliff” conversation: media coverage often circles around age 35, but fertility doesn’t drop off in one clean step. It’s influenced by multiple factors for both partners. If age anxiety is driving your choices, it may help to focus on what you can control this cycle: timing and consistency.
Supplies checklist: keep it clean, calm, and repeatable
You don’t need a drawer full of gadgets. You need a setup you can repeat without improvising mid-attempt.
- LH ovulation test strips (or digital tests)
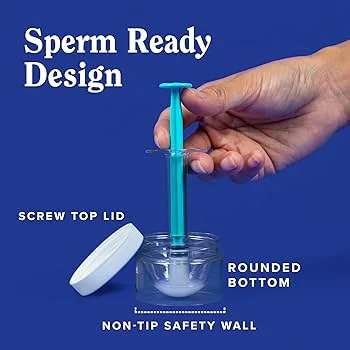
- Clean collection container (if collecting at home)
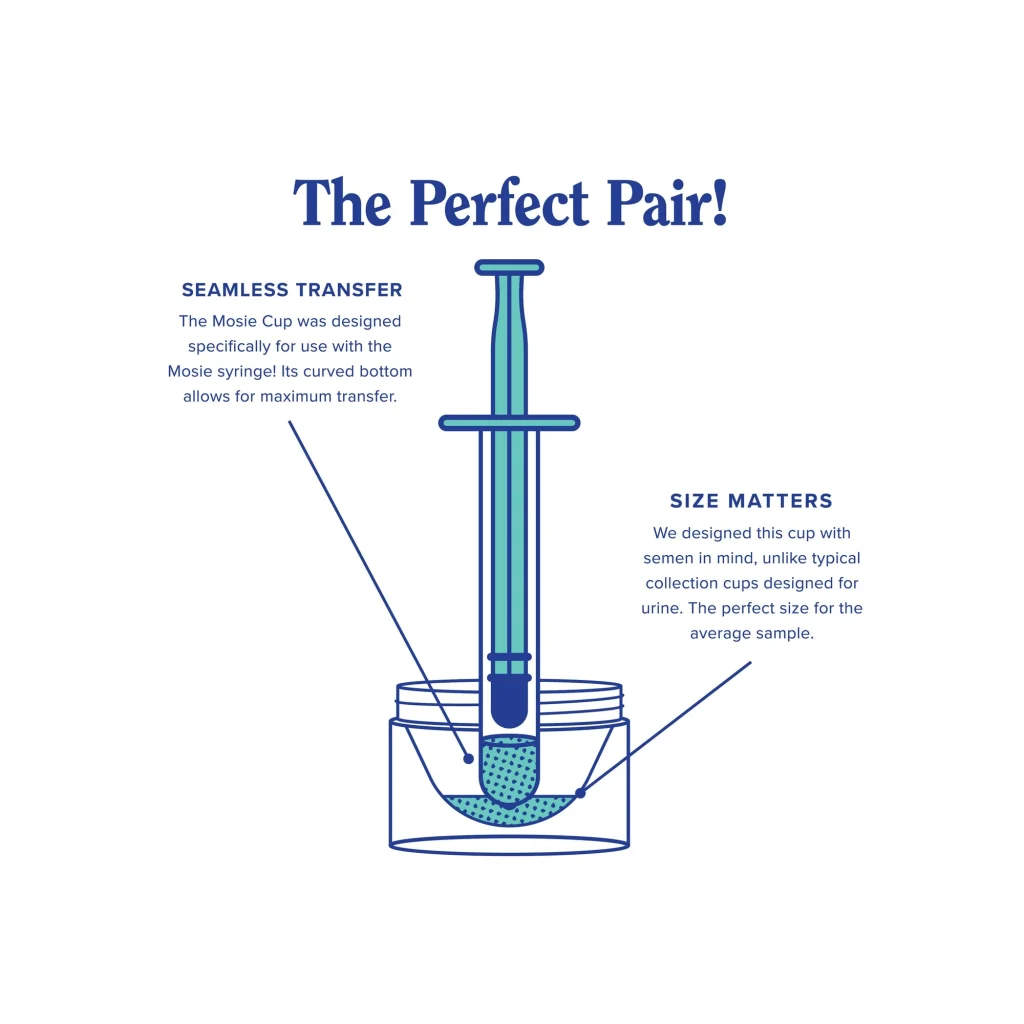
- Needleless syringe or cervical insemination syringe (designed for ICI)
- Optional: menstrual disc (some people use it to help keep semen near the cervix)
- Clean towel, tissues, and a timer
If you’re shopping specifically for an all-in-one option, a at-home insemination kit for ICI can reduce last-minute substitutions and help standardize your routine.
Step-by-step: an ICI attempt at home (plain language)
This is the “doable” version. If anything feels painful or unsafe, stop and consider talking with a clinician.
1) Confirm you’re in the window
Look for an LH surge and/or fertile-type cervical mucus. If you track basal body temperature, remember it confirms ovulation after the fact, so it’s not your main timing tool for ICI.
2) Prep your space (and your brain)
Wash hands. Lay out supplies. Set a timer. Keep the mood neutral if that helps. Plenty of people conceive without it feeling like a movie scene.
3) Collect and transfer promptly
Follow the instructions for your supplies. In general, you want a gentle transfer near the cervix, without force. Go slowly and avoid introducing air.
4) Rest briefly if you want
Many people lie down for comfort for 10–20 minutes. It’s not a magic trick. It’s just a calm finish to the attempt.
5) Log what happened
Write down the day, LH result, and time. That small note helps you improve timing next cycle without re-litigating every detail.
Mistakes that waste a cycle (and how to avoid them)
Chasing the wrong day
Trying too early “just in case” can miss the real window. Build your plan around the LH surge and your typical cycle pattern.
Overcomplicating the process
Switching tools every month makes it harder to learn what works for your body. Keep your method consistent for a few cycles.
Ignoring legal and documentation realities with a known donor
Recent coverage of a Florida case has reminded many families that donor intent and legal status can be complicated, especially outside a clinic setting. If you’re using a known donor, consider getting informed before you start—paperwork and local rules can matter more than people expect.
To read more about that general topic, see: Florida Supreme Court makes ruling in at-home artificial insemination case.
Letting pop culture set your expectations
TV loves surprise pregnancies and tidy timelines. Some shows even write real-life pregnancies into the plot, which makes it look effortless. Real cycles are messier. A better benchmark is “well-timed attempts,” not a scripted arc.
FAQ: fast answers before you try again
What if my cycles are irregular?
Use LH testing and cervical mucus rather than calendar counting. If cycles are very unpredictable, a clinician can help assess why.
How many times should we inseminate in a cycle?
Many people aim for 1–2 attempts in the fertile window. More isn’t always better if it increases stress or pushes you outside the window.
Can stress “ruin” the cycle?
Stress can affect sleep, libido, and consistency. It doesn’t automatically prevent pregnancy, but it can make timing harder to execute.
Next step: make your next attempt simpler
If you want a repeatable setup that supports good timing, start with a purpose-built at-home insemination kit for ICI and a basic LH testing plan. Keep notes for one cycle. Adjust one variable at a time.
How does at-home insemination (ICI) work?
Medical disclaimer: This article is for general educational purposes only. It does not provide medical advice, diagnosis, or treatment. For personalized guidance—especially if you have pain, known reproductive conditions, or repeated unsuccessful cycles—consult a licensed healthcare professional.