


Myth: At-home insemination is only something people try when they’re “out of options.”
Reality: Many people start with ICI because it’s private, lower-intervention than IVF, and easier to repeat across multiple cycles.

Right now, fertility talk is everywhere. Celebrity pregnancy announcements and “baby year” roundups keep the conversation in the spotlight. At the same time, news about reproductive rights disputes and the ongoing debate about the so-called “fertility cliff” has people asking practical questions: What can I do at home, and what actually matters?
What people are talking about (and why ICI keeps coming up)
When celebrity baby news hits, it tends to glamorize the outcome and skip the process. That gap sends real people searching for realistic paths, including at-home insemination (ICI). Social feeds also amplify the number “35,” which can create pressure even though fertility doesn’t flip like a switch on a birthday. It’s more gradual and depends on several factors for both egg and sperm.
Another trend: tool-driven decision-making. People track ovulation, compare home options to IVF, and look for ways to reduce guesswork. It’s the same mindset behind using apps and even home insemination kit searches to understand predictions and probabilities. In fertility, better inputs (timing, technique, and health context) matter more than hype.
What matters medically (keep this simple)
ICI is about placing semen near the cervix around the fertile window. The goal is to give sperm a shorter trip and a better shot, without medical instrumentation.
The three factors that move the needle
Timing: This is the biggest lever. ICI works best when it’s close to ovulation. Ovulation predictor kits (OPKs) and cervical mucus changes are common tools.
Sperm handling: Temperature swings, delays, and contamination can hurt viability. A calm, clean, quick process helps.
Underlying barriers: Irregular ovulation, known tubal issues, or significant sperm concerns may limit what ICI can do. That’s when testing and clinical options become more relevant.
Quick safety note
Use sterile or single-use components where possible, avoid sharp or improvised tools, and never insert anything that can damage tissue. If you have pelvic pain, fever, unusual discharge, or bleeding that worries you, pause and contact a clinician.
How to try ICI at home (tools, technique, comfort, cleanup)
This is the practical part. Keep the setup boring. Boring is good.
1) Get your space ready (before timing gets intense)
- Wash hands and clear a clean surface.
- Have tissues, a towel, and a small trash bag nearby.
- Plan for privacy and a 15-minute buffer so nobody feels rushed.
2) Choose the right tools
A purpose-built home insemination kit for ICI typically includes items designed for safer transfer and less mess. Avoid needles or anything sharp. If you’re unsure whether a tool is body-safe, don’t use it.
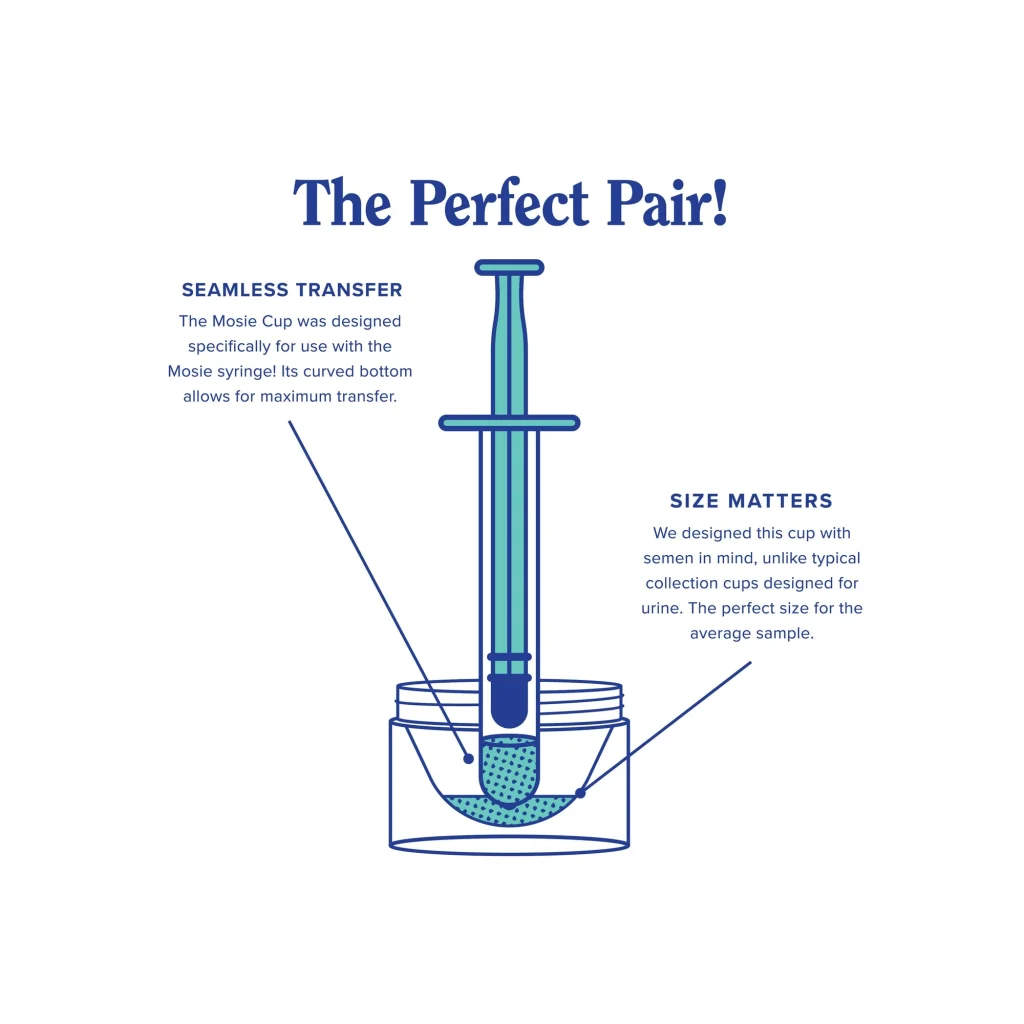
3) Collection and transfer: keep it gentle and quick
- Collect semen into a clean container (follow any donor bank instructions if applicable).
- Draw it into the syringe slowly to reduce bubbles.
- Insert the syringe only as far as comfortable (shallow placement is typical for ICI).
- Depress the plunger slowly. Rushing can cause discomfort and leakage.
4) Positioning that people actually tolerate
You don’t need a gymnastics routine. Most people choose one of these:
- On your back with a pillow under hips for comfort.
- Side-lying if back-lying is uncomfortable.
- Feet up on a chair only if it helps you relax (not because it’s required).
Rest 10–20 minutes if it feels right. Stressing about the clock can backfire.
5) Cleanup without over-cleaning
- Expect some leakage afterward. That’s normal.
- Avoid douching or internal washing.
- Dispose of single-use items and wash reusable items as directed by the manufacturer.
When to seek help (and what to ask for)
At-home ICI is a reasonable starting point for many people, but it shouldn’t become an endless loop if something is off.
Consider getting fertility support if:
- You’re under 35 and have tried for about 12 months without pregnancy.
- You’re 35+ and have tried for about 6 months without pregnancy.
- Cycles are very irregular, very long, or ovulation is hard to confirm.
- You have a history of pelvic inflammatory disease, endometriosis, or tubal concerns.
- There’s known sperm-related concern (count, motility, or collection issues).
Useful, specific questions to bring to a clinician
- “Can we confirm whether I’m ovulating, and roughly when?”
- “Should we do basic labs and an ultrasound?”
- “Is there any reason ICI would be low-yield for my situation?”
- “What would change the plan: IUI, medicated cycles, or IVF?”
Medical disclaimer
This article is for general education and does not replace medical advice. It does not diagnose or treat any condition. If you have health concerns, pain, signs of infection, or questions about donor sperm, medications, or legal/consent considerations, consult a qualified clinician or local professional.
Next step: make your first attempt calmer (not louder)
If you want a straightforward setup that supports clean transfer and less fumbling, start with a kit designed for ICI and a simple plan for timing.