




You’ve probably noticed it: pregnancy news is everywhere. Between celebrity announcement roundups, TV plotlines that hinge on “surprise” conception, and constant debates about family-building rights, it can feel like everyone has an opinion.

But your cycle doesn’t care about the headlines. It cares about timing.
Thesis: If you’re considering ICI, the smartest plan is a simple if/then decision path that prioritizes ovulation timing, safe setup, and clear next steps.
Start here: what at-home insemination (ICI) is—and isn’t
Intracervical insemination (ICI) is an at-home method that places semen at or near the cervix, typically using a syringe-style applicator designed for this purpose. It’s different from clinic procedures like IUI and IVF.
ICI can appeal to people who want privacy, lower costs, or a first-step option before moving to clinical care. It’s also common for solo parents by choice and LGBTQ+ family building.
Medical disclaimer: This article is educational and not medical or legal advice. It doesn’t diagnose conditions or replace care from a licensed clinician. If you have severe pain, fever, unusual discharge, or heavy bleeding, seek medical care promptly.
The decision guide: If…then… your next move
If you’re early in the process, then make timing your “main character”
Celebrity pregnancy chatter can make conception sound instant. Real life is more methodical. Your best leverage is inseminating close to ovulation.
If your cycles are fairly predictable, then track ovulation with LH strips and watch for the surge. Many people target the day of the surge and the next day.
If your cycles vary a lot, then start testing earlier than you think you need to. Consider adding basal body temperature tracking to confirm that ovulation likely happened, since LH predicts a surge but doesn’t guarantee release.
If you want the simplest routine, then use a two-step timing plan
Overcomplication is the fastest way to burn out. Keep it tight.
- Step 1: Identify your likely fertile window (cycle history + LH testing).
- Step 2: Plan ICI for the LH surge day and/or the day after.
If you can only pick one attempt, aim for the surge day or the next day, depending on your pattern and how quickly your tests turn positive.
If you’re choosing a home insemination kit, then prioritize safety and comfort
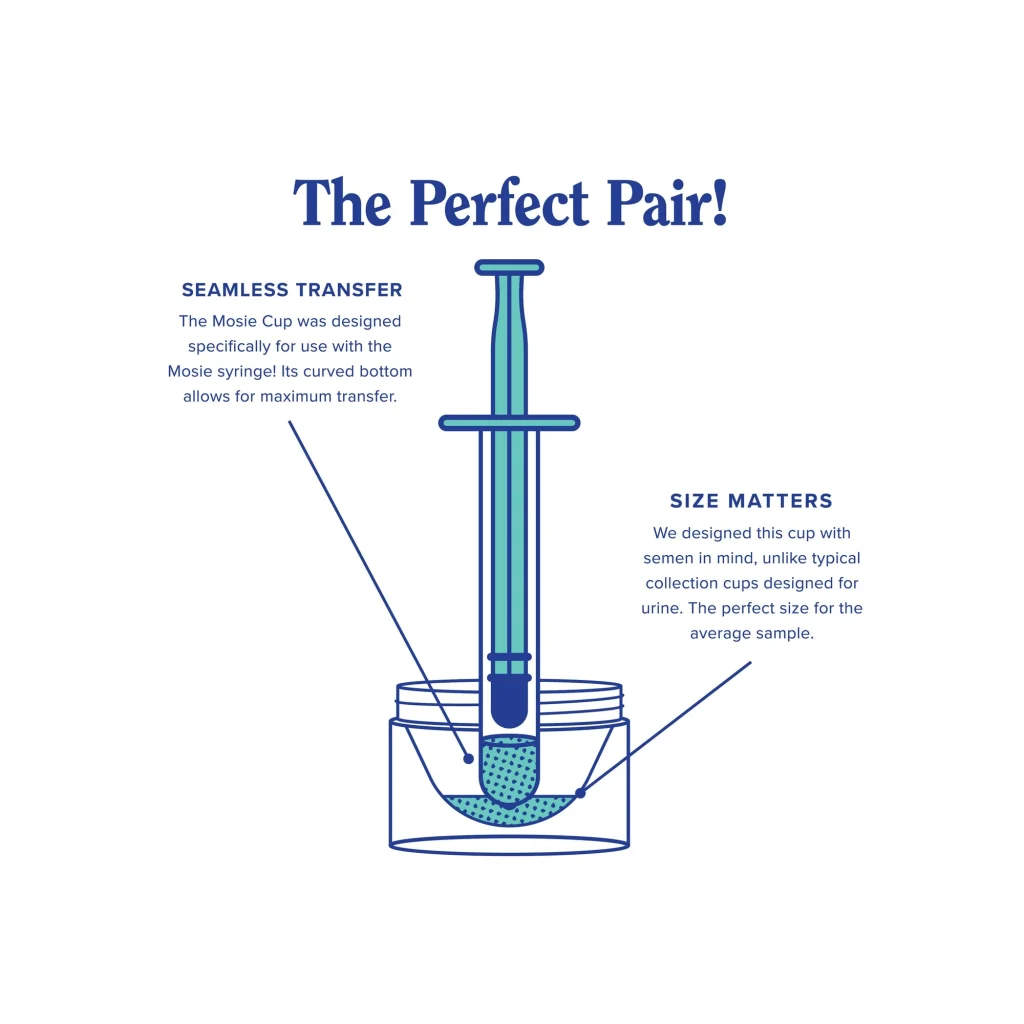
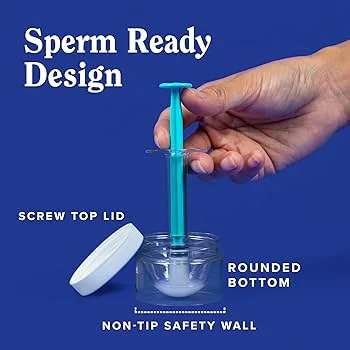
A home insemination kit should help you do the basics well: controlled placement, clean handling, and less irritation. Skip anything that isn’t intended for vaginal use.
If you’re tempted to DIY with random syringes or household items, then pause. Tissue irritation and contamination risk aren’t worth it.
If you want a purpose-built option, then look for a kit that emphasizes sterile or hygienic packaging, smooth edges, and easy handling. Here’s a relevant option to compare: at-home insemination kit for ICI.
If you’re using a known donor, then don’t ignore the legal side
Family-building is in the cultural spotlight right now, and not just because of celebrity news. Legal decisions and policy debates can shape what happens when agreements are informal.
If you’re working with a known donor, then consider getting legal guidance before insemination. Some recent reporting has highlighted that donor intent may not automatically determine parental rights in at-home arrangements.
To read more context, see this coverage via Florida Supreme Court makes ruling in at-home artificial insemination case.
If you’ve tried a few well-timed cycles, then decide whether to adjust or escalate
It’s normal to want a quick “IVF alternative.” Still, ICI and IVF aren’t interchangeable. Think of ICI as a first-line home option, not a replacement for medical evaluation when you need it.
If attempts haven’t been well-timed, then fix timing first. A perfect kit can’t outrun a missed fertile window.
If you’ve had several well-timed tries with no success, then consider a clinician visit to discuss labs, ovulation, semen parameters, or whether IUI/IVF makes more sense for your situation.
Quick FAQ
Is ICI the same as IUI?
No. ICI is typically at-home placement near the cervix. IUI is usually done in a clinic and places washed sperm into the uterus.
When is the best time to do ICI?
Most people aim for the day of the LH surge and/or the next day. Timing is the biggest controllable factor.
Do I need a home insemination kit to do ICI?
You don’t “need” one to understand the method, but a purpose-made kit can improve comfort and reduce avoidable irritation or contamination risk.
How long should I try at-home insemination before seeing a clinician?
Many people seek guidance after several well-timed cycles, sooner if cycles are irregular, you have known fertility concerns, or anything feels painful or abnormal.
Does a sperm donor automatically give up parental rights with at-home insemination?
Not always. Rules vary by location and circumstances. Consider legal advice and documentation before you start.
CTA: Keep it simple, keep it timed
If you’re ready to plan your next cycle, focus on two things: (1) identify the LH surge and (2) use a clean, comfortable setup you can repeat.
How does at-home insemination (ICI) work?
Note: This content is for general education only and is not medical or legal advice. For personalized guidance, consult a licensed healthcare professional and, when needed, a qualified attorney in your area.

